All published articles of this journal are available on ScienceDirect.

CD14 Gene Variants and Susceptibility to Helicobacter pylori-Associated Gastropathies in Iraqi Patients
Authors Info & Affiliations
Abstract
Introduction
Helicobacter pylori (H. pylori) is a gram-negative bacterium that colonizes the gastric mucosa and is implicated in a range of gastrointestinal disorders.
Methods
From September 2024 to January 2025, a cross-sectional study was conducted at the Al-Hakim General Hospital/Digestive System Center in Iraq. 50 patients and 25 healthy persons (35 females and 40 males) aged 21 to 70 years were among the 75 specimens collected.
Results
Among the 75 participants, 50 were gastric patients and 25 were controls. All patients tested positive for H. pylori using the one-step Ab/Ag test, with 46% showing positive antibodies and 42% positive antigens. CD14 levels were markedly higher in patients (120.8 pg/ml) compared with controls (12.3 pg/ml). However, the genotyping of CD14 revealed three genotypes: CC, CT, and TT represented (16%, 60% and 24%) respectively in patients compared with the control group, where the frequencies were (72%, 20% and 8%) respectively. The CT genotype was more common among patients suffering from gastropathies, while the CC genotype was more frequent in healthy controls. Serum sCD14 levels were higher in TT and CT carriers compared with CC (160.7 ± 0.43: 120.9 ± 47.44 vs. 80.9 ± 3.59; P = 0.003**).
Discussion
The increased prevalence of CT and TT genotypes among patients, alongside elevated sCD14 levels, suggests that the T allele may enhance inflammatory responses and increase susceptibility to gastropathies.
Conclusion
These findings indicate that CD14 polymorphisms are significantly associated with H. pylori-related gastropathies in the Iraqi population (P < 0.05).
1. INTRODUCTION
Helicobacter pylori (H. pylori) is a gram-negative and spiral-shaped bacterium that survives in the stomach epithelium of humans. More than half of the world's inhabitants are thought to be sick with H. pylori, yet only a slight percentage of people have clinically severe gastropathies. The spectrum of diseases associated with H. pylori includes chronic gastritis, peptic ulcer disease, mucosa-associated lymphoid tissue (MALT) lymphoma, and gastric adenocarcinoma. The variability in disease outcomes is influenced by multiple factors, including bacterial virulence, environmental exposures, and, most notably, host genetic predispositions [1].
One of the key components of the host’s innate immune system is the pattern recognition receptor (PRR) family, which plays a central role in recognizing pathogen-associated molecular patterns (PAMPs) and initiating early immune responses. CD14, a member of this receptor family, is expressed on the surface of macrophages, neutrophils, and monocytes, where it acts as a coreceptor for bacterial lipopolysaccharide (LPS), a key constituent of the outer membrane of Gram-negative bacteria, including H. pylori. CD14 can also exist in a soluble form (sCD14), which has immunomodulatory effects [2].
Genetic variations within the CD14 gene, especially single-nucleotide polymorphisms (SNPs) in its promoter region, have been shown to influence CD14 expression levels and modulate immune responses. Among these, the C-159T polymorphism (rs2569190) has been extensively studied due to its association with increased expression of CD14 and altered cytokine profiles. This SNP has been linked to a heightened inflammatory response, which could affect the severity and type of gastropathy resulting from H. pylori infection [3].
Although CD14 polymorphisms have been studied in several populations, to our knowledge, this is the first study in an Iraqi cohort. Population-specific data are essential to understand genetic variability and its clinical implications in this region.
This study aims to explore the association between CD14 gene polymorphisms and susceptibility to H. pylori-related gastric diseases, highlighting their potential role as immunogenetic modulators. Understanding these genetic influences could contribute to the development of personalized diagnostic and therapeutic approaches in managing H. pylori infections and their complications.
2. MATERIALS AND METHODS
A total of 75 subjects were recruited for this study and were divided into two study groups: Group-I patients (n = 50), Group-II controls (n = 25), in Al-Hakim General Hospital / Digestive System Center and at various private clinics, Iraq, during the period from September 2024 to January 2025. For each subject, both physical and clinical examinations were performed, and the information was recorded in a data sheet. This research was conducted in accordance with the ethics of the Al-Hakim General Hospital / Digestive System Center and the affiliated private clinics, Iraq. All respondents received verbal informed consent. Blood specimens were gathered for ELISA and CD14C-159T (rs2569190) gene polymorphism PCR amplification. For blood sampling and storage, venous blood (5 mL) was collected into EDTA and plain tubes. After disinfection with 70% alcohol, 2 ml were placed in EDTA tubes and stored at 4°C and processed within 6 hours for DNA extraction, while the remaining 3 ml were used for serum tubes and were centrifuged at 3,000 rpm for 10 minutes, and serum aliquots were stored at −20°C until ELISA for sCD14.
The control group consisted of 25 clinically healthy individuals recruited from the same catchment area as the patients and matched to them by age and sex to minimize confounding effects. All controls tested negative for Helicobacter pylori infection using both the rapid urease test and PCR assay. They reported no gastrointestinal symptoms and had no history of gastritis, peptic ulcer disease, or other gastrointestinal disorders. Individuals with autoimmune or systemic inflammatory diseases, as well as those who had received antibiotics or proton pump inhibitors within the previous four weeks, were excluded from participation.
2.1. Estimation of Serum Cytokines and Biomarkers
The levels of CD14 were determined according to the manufacturer's instructions (Elabscience, China).
2.2. DNA Extraction and PCR
The CD14 gene is located on chromosome 5q31.1. The −159 C→T (rs2569190) polymorphism lies within the promoter region and has been reported to affect transcription factor binding and CD14 expression. Using the commercially available G-spinTM Total DNA Extraction Kit (Intron-bio, USA), genomic DNA was extracted from fresh peripheral blood (2 ml in EDTA) and stored at -20 °C until required. Single-nucleotide polymorphisms (SNPs) linked to CD14C-159T (rs2569190) were defined utilizing Polymerase chain reaction with TARMS-PCR primers in 4 primers responses utilizing forward outer primer: 5′-TTCTTTCCTACACAGCGGCA CCC-3′; reverse outer primer: 5′-TTGGTGCCAACAGAT GAGGTTCAC-3′; forward inner primer: 5′-CTGCAGAATCC TTCCTGTTACGAC-3′ and reverse inner primer: 5′-TGTAGGATGTTTCAGGGAGGGGTA-3′ [4] with an amplicon product of Common product size: 561 for Control; 384 for C alleles; 277 for T alleles and 277 and 384 for TC alleles. The reaction mix (25 μL) included 7 μL DNA template, 12.5 μL master mix (Promega, USA), 4 μL primers (1 μL for each), and 1.5 μL Nuclease Free Water (USA Applied PCR System). Afterward, 5 min of amplification at 95 oC, there were 35 cycles of 95 oC for 30 seconds, 57 oC for 35 seconds, and 72 oC for 45 seconds, and finally a final extension at 72 °C for 10 min. A Cleaver gel documentation system (Biometer, Germany) was recycled to observe PCR results after electrophoresis on 1.5% agarose gels and staining with ethidium bromide.
To ensure reproducibility, 10% of the samples were randomly selected and re-genotyped in a blinded fashion; concordance between original and repeat genotypes exceeded 99%. Samples or variant assays with call rates below 95% were excluded from downstream analysis. Hardy–Weinberg equilibrium was tested in the control group for each SNP, and variants with significant deviation (P < 0.001) were inspected for genotyping error and, if unresolved, removed from association analyses.
2.3. Statistical Analysis
All statistical analyses were performed using SPSS version and GraphPad Prism [insert version]. Genotype and allele frequencies were compared between patients and controls using the chi-square test or Fisher’s exact test when appropriate. The strength of association was expressed as odds ratios (ORs) with corresponding 95% confidence intervals (CIs). For multiple comparisons across CD14 polymorphisms, Bonferroni correction was applied to adjust the significance threshold (adjusted P = 0.05 / number of tests). Associations with corrected P values < 0.05 were considered statistically significant [5].
Continuous variables were expressed as mean ± standard deviation (SD) and compared using Student’s t-test. Hardy–Weinberg equilibrium was tested for all SNPs in the control group. Effect sizes were calculated using ORs, while confidence intervals were used to indicate the precision of each estimate.
3. RESULTS AND DISCUSSION
3.1. Distribution of Patients According to Sex
The present study included 75 samples, divided into two groups: patients = 50 (66.7%) and controls = 25 (33.3%) at Al-Hakim General Hospital / Digestive System Center and various private clinics in Iraq. The study shows that the number of male patients was higher than the number of female patients, with 40 (53.3%) and 35 (46.7%), respectively.
The higher prevalence of H. pylori-associated gastropathies among male subjects aligns with findings from similar Middle Eastern cohorts. For instance, reported that 54.5% of H. pylori-positive peptic ulcer patients in Iraq were male (p < 0.05) [6]. This male predominance is thought to arise from several factors: biological differences; male hormonal profiles, especially lower estrogen levels, may reduce mucosal protection against gastric injury and inflammation [6]. Lifestyle patterns: Men may have greater exposure to risk factors like smoking, alcohol use, or occupational hazards, which can increase susceptibility to H. pylori-related disease [7]. Health-seeking behavior: Cultural norms may delay women's presentation for medical assessment, reducing their representation in hospital-based studies.
Nevertheless, some studies show no clear sex differential. For example, research in Zakho City, Iraq, found no significant infection rate difference between genders (p not significant) [8]. Likewise, meta-analysis and systematic review concluded that gender is not a consistent risk factor for H. pylori infection [9].
Thus, while our results support a male predominance among patients, it is essential to consider regional and methodological variations. Future research should control for variables such as smoking, alcohol consumption, and socioeconomic status to better understand this disparity.
3.2. Age Distribution
The patient groups were divided into five categories according to their age ranges. The highest frequency of patient age was in 41-50, followed by 51-60, 31-40, and 61-70; the lowest frequency was in 21-30, with 20, 10, 9, 8, and 3, respectively. While in control, age was in 41-50, followed by 51-60, 31-40, 61-70, and the lowest frequency was 21-30, with 14, 5, 4, 1, and 1, respectively.
The present study revealed that the highest frequency of Helicobacter pylori infection occurred in the 41–50 age group among both patients and controls, with a gradual decrease in prevalence toward the younger (21–30) and older (61–70) age groups. This age-related distribution aligns with global findings indicating that H. pylori infection is typically acquired in early childhood and persists throughout life, leading to a cumulative increase in prevalence with age until midlife [10]. The decline in the oldest group may be due to age-related gastric atrophy or to prior successful eradication therapy. Furthermore, older age groups, particularly those born before widespread improvements in hygiene and sanitation, are more likely to have been exposed to H. pylori during early life, a phenomenon known as the birth cohort effect [9]. Additionally, the lower infection rates among younger individuals may reflect enhanced living standards, better water quality, and increased awareness of personal hygiene in recent decades. Therefore, the age distribution observed in this study is consistent with epidemiological patterns reported in both regional and international studies.
3.3. Rapid Diagnostic Test (RDT)
Serum from all 50 patients was tested using this method to detect H. pylori Ab and Ag simultaneously. Table 1 displays the percentage of patients whose Ab test was positive (23/50, 46%) and negative (27/50, 54%) out of 50 total patients. In contrast, 21 (42%) and 29(58%) were negative for (Ag) among patients. There was a significant difference between the two groups (p<0.001) as shown in Table 1.
| P value= 0.001*** | 23(46%) | Positive | Ab | Rapid Diagnostic Test |
| 27(54%) | Negative | |||
| 21(42%) | Positive | Ag | ||
| 29(58%) | Negative |
The findings of the current study indicate that rapid diagnostic tests (RDTs) demonstrated a detection rate of 61.29% for Helicobacter pylori infection, as shown in Table 1, which is consistent with previous reports [11]. Internationally, the positivity rate of RDTs for H. pylori ranges from 61% to 87%, reflecting differences in test accuracy across populations and regions [12, 13]. These variations can be attributed to individual immune responses and the duration of infection, which influence the test's ability to detect bacterial antigens effectively [14]. Moreover, because RDTs may not differentiate between active and past infections, their sensitivity and specificity can be compromised, increasing the likelihood of false-positive results [15].
A previous study [15] conducted in Ramadi, Iraq, found a slightly higher positivity rate of 67% among patients presenting with gastrointestinal symptoms at local teaching hospitals. This difference may be explained by treatment interventions received by some patients before testing, which may have lowered antigen levels and affected test performance. Additionally, stool antigen tests (SATs), often used in initial diagnosis and public health screening due to their cost-effectiveness, are influenced by factors such as local test quality, laboratory sensitivity, and patient condition [16]. The present findings align with the broader literature, underscoring the need for careful interpretation of RDT results within clinical and epidemiological contexts.
3.4. Molecular and Immunological Study
3.4.1. Distribution of CD14C-159T (rs2569190) Gene Polymorphism
The results of detection polymorphism in the CD14C-159T (rs2569190) locus show there are three genotypes, GG, GA, and AA, with band sizes of 561, 384, and 277 bp, as shown in Fig. (1) for patients and control groups.
The genotypes frequency in patients was as follow; CC (16%), CT (60%) and TT (24%); while in the control subjects; CC (72%), CT (20%) and TT (8%), Table 2, that show increase significant differences between all genotype and Allele frequency at P-value ≤ 0.05.
| P-value | OR(95% CI) | Cntrol | Patients | CD14 |
|---|---|---|---|---|
| n=25 | n=50 | |||
| 0.0026* | 0.0654(0.0179 to 0.2381) | (18)72% | (8)16% | C/C |
| 0.0054** | 8.163(1.636 to 24.52) | (5)20% | (30)60% | C/T |
| < 0.0001*** | 10.782(0.9514 to 65.18) | (2)8% | (12)24% | T/T |
| < 0.0001*** | 11.44 (3.078 to 23.71) | 41 (82%) | 46 (46%) | C allele |
| 0.251(0.04217 to 0.3249) | 9 (18%) | 54 (54%) | T allele |
Note: p≤ 0,05, OR: Odds Ratio, CI: Confidence Interval
The analysis of the CD14 C-159T (rs2569190) promoter polymorphism revealed a significant difference in genotype distribution between patients and controls, with the CT genotype being the most prevalent among patients (60%), followed by TT (24%) and CC (16%). In contrast, the control group exhibited a predominance of the CC genotype (72%), with lower frequencies of CT (20%) and TT (8%) Table 2. This statistically significant variation (P ≤ 0.05) suggests a potential association between the presence of the T allele and increased susceptibility to Helicobacter pylori-associated gastropathies. The T allele has been linked to elevated CD14 expression, enhancing monocyte activation and proinflammatory cytokine production, thereby intensifying the host’s inflammatory response to H. pylori infection [17]. This heightened immune activation may contribute to mucosal damage and increased disease severity. Several studies have confirmed that individuals carrying the CT or TT genotypes are more prone to developing gastric inflammation and other related disorders, emphasizing the immunogenetic role of CD14 in H. pylori pathogenesis [18]. Therefore, the observed genotype distribution in this study supports the hypothesis that the C-159T polymorphism in the CD14 gene is a genetic risk factor for susceptibility to H. pylori-induced gastrointestinal diseases.
The present study also observed that the concentration of CD14 (pg/mL) in patients was 120.8 ± 12.11 pg/mL and increased significantly compared with normal individuals, whose levels were 12.3 ± 1.36 pg/mL as shown in Table 3.
| Control | Patients | CD14 |
|---|---|---|
| 12.3 ± 1.36 | 120.8 ± 12.11 | Mean ± std. Deviation |
| ˂ 0.000 *** | P-value | |
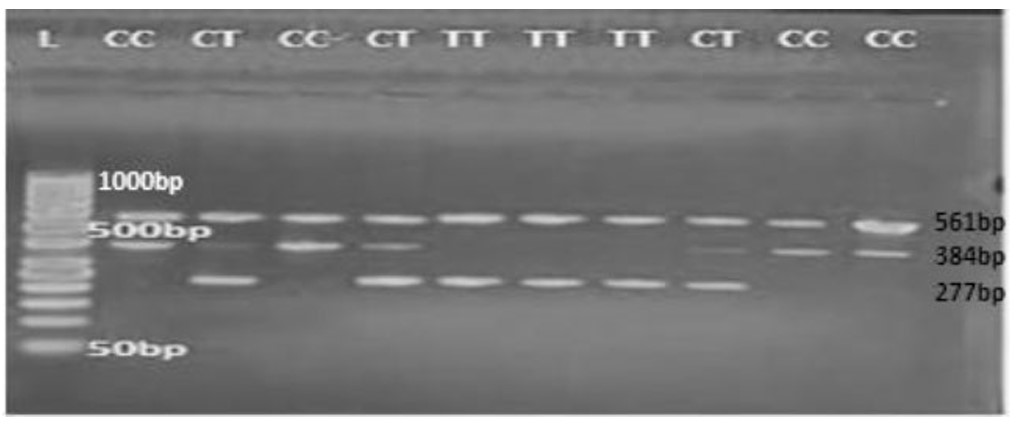
Representative gel electrophoresis showing TARMS-PCR results for CD14 C−159T genotypes: Lane 1 = marker; Lanes 2,4,10 and 11 = CC genotype; Lanes 3, 5 and 8 = CT genotype; Lanes 6–8 = TT genotype, agarose gel 1%, 80 vol. 1.30 hour.
The current study demonstrated a significantly elevated concentration of soluble CD14 (sCD14) in patients with Helicobacter pylori-associated gastropathies (120.8 ± 12.11 pg/mL) compared to healthy controls (12.3 ± 1.36 pg/mL), as shown in 3. This marked increase suggests an enhanced innate immune response triggered by Table H. pylori infection, as CD14 is a key co-receptor for recognizing bacterial lipopolysaccharides (LPS), particularly in gram-negative bacteria such as H. pylori [19]. Elevated sCD14 levels have been reported in various inflammatory conditions and are thought to reflect monocyte/macrophage activation, which contributes to mucosal inflammation and tissue damage in the gastric lining [20]. Furthermore, CD14 expression is influenced by genetic variations such as the C-159T polymorphism, where the T allele is associated with higher transcriptional activity and increased sCD14 production [17]. The significantly higher levels observed in patients may therefore reflect both a genetic predisposition and the ongoing immunological challenge posed by chronic H. pylori infection. Recent studies have confirmed that elevated sCD14 serves not only as a biomarker of infection but also correlates with disease severity and progression in gastrointestinal disorders [18]. These findings support the role of CD14 in mediating inflammatory responses in H. pylori-related diseases and highlight its potential as a diagnostic and prognostic indicator.
This result also explains that a high production level of CD14 occurs in the homozygous mutant type TT, followed by heterozygous CT, while low production occurs in the homozygous CC. This result shows significant differences among genotypes, as shown in Table 4, which indicates that the CC genotype of the CD14C-159T (rs2569190) polymorphism in the studied population is associated with a good prognosis with respect to low serum CD14 production.
| TT | CT | CC | Genotype |
|---|---|---|---|
| 160.7 ± .43 | 120.9 ± 47.44 | 80.9 ± 3.59 | Patients |
| 15 ± 1.04 | 14.3 ± 5.12 | 7.6 ± 0.075 | Control |
| ˂ 0.003 ** | 0.008 ** | ˂ 0.0232 * | P-value |
The findings of this study indicate that individuals carrying the TT genotype of the CD14 C-159T (rs2569190) polymorphism exhibited the highest levels of serum CD14, followed by those with the CT genotype, while individuals with the CC genotype had significantly lower CD14 concentrations, as detailed in Table 4. These differences were statistically significant, suggesting a strong association between the CD14 genotype and the regulation of soluble CD14 expression. The T allele has been previously associated with increased promoter activity, leading to higher transcription rates and elevated sCD14 production [21]. Consequently, individuals with the TT genotype are more likely to experience heightened inflammatory responses due to increased monocyte activation in response to bacterial components such as H. pylori lipopolysaccharides [19]. In contrast, the CC genotype appears to confer a more controlled immune response, potentially resulting in better clinical outcomes and a lower risk of chronic inflammation or tissue damage. This aligns with previous research suggesting that the C allele is linked to a more regulated innate immune activation and may be protective in inflammatory and infectious diseases [20, 17]. Therefore, the observed genotype expression relationship supports the role of CD14 polymorphisms not only in susceptibility to infection but also in modulating disease severity and prognosis.
CONCLUSION
This study demonstrates a significant association between the CD14 C-159T (rs2569190) gene polymorphism and the host immune response to Helicobacter pylori infection. The presence of the T allele, particularly in individuals with the TT and CT genotypes, was associated with higher serum levels of soluble CD14, suggesting an enhanced inflammatory response and increased susceptibility to H. pylori-related gastropathies. Conversely, the CC genotype was more frequent among healthy controls and was linked to lower CD14 expression, suggesting a possible protective effect. Overall, these findings support the potential utility of CD14 polymorphisms as immunogenetic indicators for identifying individuals at increased risk of gastric diseases and may guide future research toward personalized diagnostic and therapeutic approaches. Larger multicenter studies and functional analyses are warranted to validate these associations and to assess the clinical utility of CD14 genotyping in risk stratification and personalized management.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: A.A.S.: Original draft preparation was done; A.R.M.: Methodology was designed; R.K.S.: Analysis and interpretation of results were performed; and A.A.O.: Validation was carried out. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| MALT | = Mucosa-Associated Lymphoid Tissue |
| SATS | = Stool Antigen Tests |
| RDTS | = Rapid Diagnostic Tests |
| ORS | = Odds Ratios |
| CIS | = Confidence Intervals |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval for this study was granted by The Ethics Committee of Al-hakim General Hospital In Najaf, Iraq (REF. NO. 37922).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all participants prior to sample collection.
AVAILABILITY OF DATA AND MATERIALS
All data generated or analyzed during this study are included in this published article.
ACKNOWLEDGEMENTS
Declared none.

